Ovulation is the moment a mature egg is released from the ovary into the fallopian tube, where it can meet sperm and become fertilized. The event takes roughly 24 hours from start to finish. In a typical 28-day cycle, ovulation occurs on day 14. But typical cycles are statistical abstractions — real bodies deviate, and the timing of ovulation varies even in people who consider their periods regular.
The process involves a sequence of hormonal changes that begin in the brain. It is not a switch that flips once a month. It is a cascade that unfolds over days. Knowing how ovulation works gives a person the ability to read their body's signals, whether they intend to conceive, avoid pregnancy, or simply understand recurring symptoms like mid-cycle pain or mood shifts.
How the ovary prepares an egg: the follicular phase
The ovary does not store eggs loose. Each immature egg lives inside a follicle — a small, fluid-filled sac. At birth, ovaries contain about one to two million follicles. By puberty, the number drops to roughly 300,000. Over a lifetime, only 300 to 500 will be ovulated. The rest undergo atresia, a natural process of degeneration.
At the start of each cycle, the pituitary gland releases follicle-stimulating hormone (FSH). FSH prompts several follicles in the ovary to grow. They begin at 2–5 millimeters in diameter. Within five to seven days, one follicle outpaces the others. It becomes the dominant follicle, capable of reaching 18–25 millimeters before rupture. The others stop growing and are reabsorbed.
The dominant follicle produces estradiol, a form of estrogen. Rising estradiol levels signal the uterine lining to thicken. They also feed back to the brain, eventually triggering a surge of luteinizing hormone (LH). The LH surge is the chemical event that makes ovulation happen.
The LH surge and the rupture: what ovulation looks like minute by minute
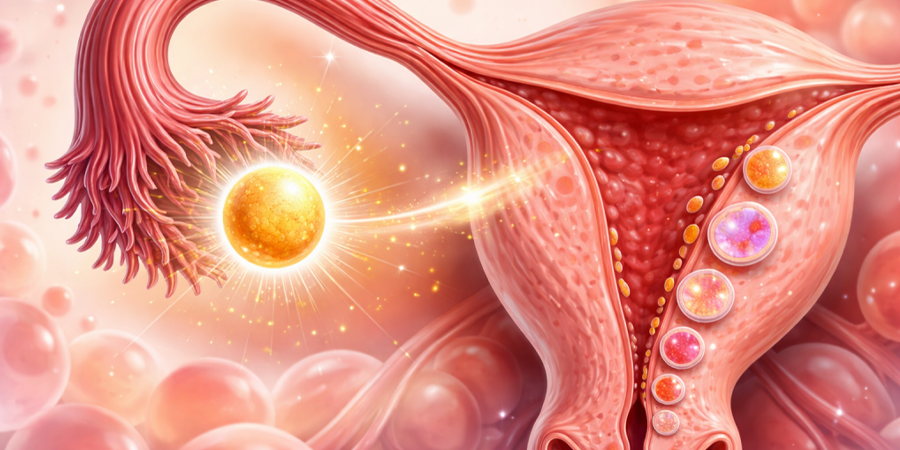
The LH surge begins about 24–36 hours before ovulation. It destabilizes the follicle wall by activating enzymes that break down collagen. The follicle swells. Its outer membrane stretches until it tears. The egg, surrounded by a cluster of supporting cells called the cumulus oophorus, is expelled into the peritoneal cavity. The fimbriae — finger-like projections at the end of the fallopian tube — sweep the egg inside.
The release is not explosive. It is a slow ooze lasting several minutes. Some people feel it. The sensation is called mittelschmerz, from the German for "middle pain." It localizes to the left or right lower abdomen, depending on which ovary ovulates. The pain lasts from a few minutes to a few hours. In a 2019 study published in Human Reproduction, 40% of participants reported ovulatory pain in at least one cycle. Most cases involved a dominant follicle larger than 20 millimeters.
Timing and the fertile window: how long the egg lives
After release, the egg survives 12 to 24 hours. Sperm, by contrast, can live in the female reproductive tract for up to five days under favorable conditions. This asymmetry creates the fertile window: intercourse in the five days before ovulation and on the day of ovulation itself can result in pregnancy. The highest probability of conception falls on the two days preceding ovulation and the day it occurs.
Several methods help identify the fertile window:
- LH urine tests. Over-the-counter strips detect the LH surge 24–36 hours before ovulation. A positive result means ovulation is imminent.
- Basal body temperature. Progesterone released after ovulation raises body temperature by 0.3–0.6°C. The shift is small, so measurement requires a thermometer accurate to two decimal places, taken every morning before getting out of bed.
- Cervical mucus. Under estrogen, mucus becomes clear, slippery, and stretchy — resembling raw egg white. This consistency facilitates sperm transport. After ovulation, progesterone makes mucus thick and opaque.
- Cervical position. During the fertile window, the cervix rises, softens, and opens slightly. Self-examination requires practice to interpret changes reliably.
- Ultrasound folliculometry. A series of transvaginal ultrasounds tracks follicle growth and confirms rupture. Used primarily in fertility treatment.
What happens after the follicle empties: the luteal phase
The empty follicle does not vanish. Under the influence of LH, it transforms into the corpus luteum, a temporary endocrine gland. The corpus luteum secretes progesterone — and, to a lesser extent, estrogen — for about 10–14 days. Progesterone stabilizes the uterine lining, making it receptive to a fertilized egg.
If pregnancy does not occur, the corpus luteum degenerates. Progesterone drops. The uterine lining sheds. Menstruation begins. If pregnancy does occur, the developing embryo produces human chorionic gonadotropin (hCG), which signals the corpus luteum to continue producing progesterone until the placenta takes over around week 8–10 of gestation.
"Ovulation is not a symptom of health. It is the sign that the complex dialogue between brain, ovary, and uterus is functioning. When that dialogue breaks, it rarely breaks silently." — Dr. Eve Feinberg, reproductive endocrinologist, Northwestern University
Anovulation and cycle disorders: when ovulation fails
Anovulation — a cycle without ovulation — occurs in roughly 10–18% of menstrual cycles in adults, and at a much higher rate in adolescents and perimenopausal people. Occasional anovulation is normal. Chronic anovulation signals an underlying condition:
- Polycystic ovary syndrome (PCOS). Affects 8–13% of reproductive-age people. High androgen levels disrupt follicle maturation. Multiple small follicles develop but none become dominant. LH is often chronically elevated, confusing the pituitary-ovarian axis.
- Hypothalamic amenorrhea. The brain downregulates GnRH pulses in response to energy deficit. Seen in athletes, people with eating disorders, or during high stress. FSH and LH drop. Follicles remain dormant.
- Hyperprolactinemia. Excess prolactin suppresses GnRH. Causes include pituitary tumors, medications, and hypothyroidism.
- Premature ovarian insufficiency. Follicle depletion before age 40. FSH is high, estradiol low. Ovulation is rare or absent.
Ovulation across the lifespan
Ovulation is not a lifelong constant. During the first 1–2 years after menarche, anovulatory cycles are common because the hypothalamic-pituitary-ovarian axis is still maturing. By the early 20s, ovulation becomes more regular. Between ages 35 and 40, the remaining follicular pool declines, and cycles shorten — the follicular phase compresses. Perimenopause, which can begin 5–10 years before the final period, features erratic ovulation interspersed with anovulatory cycles. The last ovulatory event may occur years before the last menstrual period, though pinpointing it is impossible outside prospective studies.
Ovulation detection and reproductive autonomy
Understanding ovulation is not solely a medical or fertility matter. It has practical implications for contraception, health monitoring, and the diagnosis of endocrine disorders. Before the 20th century, the timing of ovulation was unknown to science. In 1929, Kyusaku Ogino in Japan and Hermann Knaus in Austria independently identified the luteal phase as fixed at roughly 14 days, with ovulation preceding menstruation. This discovery gave rise to the rhythm method, the first systematic attempt at fertility awareness.
Modern fertility awareness methods combine multiple indicators — mucus, temperature, cervical changes — to identify ovulation with up to 99% effectiveness for contraception when used correctly, according to a 2007 study in Human Reproduction. However, typical use yields lower effectiveness, because daily tracking requires consistency and training. Apps that predict the fertile window based solely on calendar data are less reliable than methods that use real-time physiological markers.
Why ovulation matters beyond reproduction
Ovulation does more than release an egg. The pre-ovulatory rise in estradiol affects serotonin and dopamine pathways, which may explain mood and energy shifts mid-cycle. The corpus luteum's progesterone influences sleep, fluid retention, and body temperature. The ovulatory cycle is a vital sign — the American College of Obstetricians and Gynecologists recognizes it as an indicator of overall health alongside blood pressure and pulse. Regular ovulation signals that the neuroendocrine system is functioning. Its absence is a prompt to investigate.
For decades, medical research focused on menstruation while ignoring ovulation. That focus is shifting. In 2021, the US National Institutes of Health launched a large-scale prospective study tracking ovulatory function in 5,000 participants over five years, aiming to establish reference ranges and identify early biomarkers of reproductive aging. The data will shape how we understand the early warning signs of cardiovascular disease, osteoporosis, and cognitive decline — all linked to the timing of ovarian senescence.
Ovulation is not just a fertility event. It is a monthly report from the body. Reading that report is one of the most direct ways a person can assess their health, one cycle at a time.