In the first eight weeks of pregnancy, ultrasound answers a short list of questions. Is the pregnancy inside the uterus? Is there one embryo or more? Is the heart beating? The answers unfold in a predictable sequence that corresponds to embryonic development almost hour by hour. Understanding what should be visible at each week helps interpret what the scan shows — and what it cannot yet show.
Why early ultrasound exists at all
Early pregnancy ultrasound became clinically useful in the 1980s with the introduction of transvaginal transducers. The higher frequency and closer proximity to pelvic structures allowed resolution that abdominal probes could not achieve. Today, transvaginal scanning is the standard for pregnancies under 10 weeks. It visualizes structures as small as 2 millimeters.
Indications for scanning before 12 weeks include confirming intrauterine location, dating the pregnancy, investigating bleeding or pain, and assessing viability in patients with a history of miscarriage or ectopic pregnancy. In assisted reproduction, early ultrasound is routine because the exact date of embryo transfer is known, making it possible to track development with precision.
The gestational sac: week 5
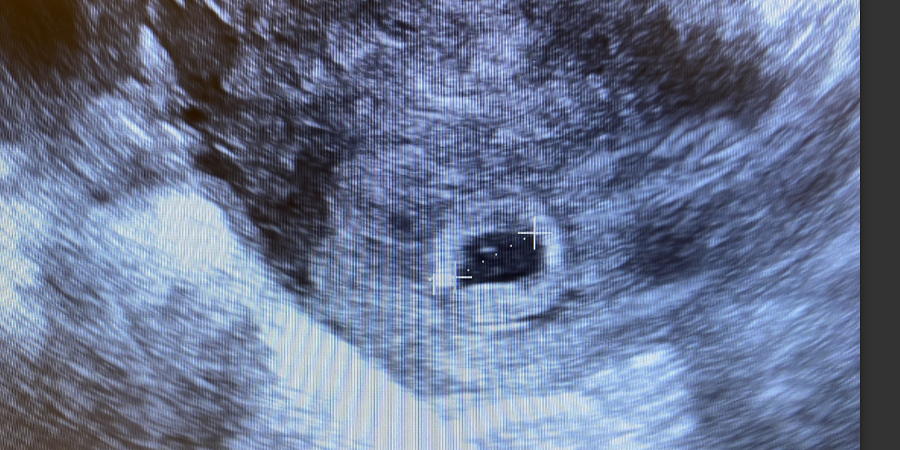
At 5 weeks — counted from the first day of the last menstrual period, which means roughly 21 days after conception — the gestational sac becomes visible. It appears as a small, black, fluid-filled circle within the thickened endometrium. The sac measures 2 to 4 millimeters in mean diameter at this stage. Its presence confirms intrauterine pregnancy and rules out an ectopic pregnancy in most cases, though a pseudosac can occasionally mimic the real thing.
The sac forms from the blastocyst cavity and is surrounded by a double ring of echogenic tissue — the decidua capsularis and decidua parietalis. This double decidual sac sign is a reliable marker of intrauterine pregnancy. Its absence raises suspicion of a pseudosac associated with ectopic pregnancy.
By 5.5 weeks, the yolk sac should appear inside the gestational sac. It looks like a small white circle, typically 3 to 6 millimeters in diameter. The yolk sac provides nutrients to the embryo before the placenta develops and is the first site of blood cell formation. Its presence confirms that the pregnancy is developing. If the gestational sac reaches a mean diameter of 20 millimeters without a visible yolk sac, the pregnancy is likely non-viable. If the sac exceeds 25 millimeters without an embryo, the diagnosis of anembryonic pregnancy is made.
"Early ultrasound is not about reassurance. It is about gathering anatomical evidence. Each week asks a specific question. The answer is visible or it is not." — Dr. Beryl Benacerraf, diagnostic radiologist, Harvard Medical School
The embryo appears: week 6
At 6 weeks, the embryo becomes visible. It sits at one pole of the yolk sac, measuring 2 to 4 millimeters in crown-rump length. The embryo at this stage is a straight or slightly curved line — no limbs, no face, no visible organs. But at its center, a flicker appears on the screen.
Cardiac activity begins between 5.5 and 6.5 weeks. The heart is a simple tube at this point, not yet folded into four chambers. It beats because pacemaker cells in the primitive atrium generate spontaneous electrical impulses. The rate is typically 90 to 110 beats per minute at 6 weeks. A heart rate below 90 at this stage carries an increased risk of miscarriage. A rate above 100 is reassuring.
Transvaginal ultrasound detects cardiac activity when the embryo reaches 2 to 4 millimeters in length. If an embryo measuring 5 millimeters has no visible heartbeat, guidelines from the Society of Radiologists in Ultrasound recommend a follow-up scan in one week before diagnosing embryonic demise. If the embryo measures 7 millimeters or more without cardiac activity, the diagnosis of miscarriage is definitive.
Rapid growth: week 7
At 7 weeks, the embryo doubles in size compared to week 6. Crown-rump length reaches 9 to 14 millimeters. The heart rate accelerates to 120 to 160 beats per minute. The heart tube has looped — a critical step that creates the asymmetry needed for four-chamber development later.
New structures appear. The amniotic cavity separates from the chorionic cavity, becoming the fluid-filled space that will surround the fetus for the rest of pregnancy. Before this separation, the embryo floats in a small space; after, it moves freely within the amnion. The rhombencephalon — the embryonic hindbrain — becomes visible as a cystic space at the back of the head. This is the fourth ventricle of the developing brain. Its appearance is normal at 7 to 8 weeks and should not be mistaken for a cystic abnormality.
The umbilical cord begins to form. Two umbilical arteries and one vein connect the embryo to the developing placenta. Doppler interrogation of the umbilical artery is not performed at this stage because the embryo's circulation is too fragile, and unnecessary energy exposure should be avoided.
Taking shape: week 8
At 8 weeks, the embryo measures 16 to 22 millimeters — roughly the size of a raspberry. The term "embryo" still applies; "fetus" begins at 10 weeks. But the appearance on ultrasound has changed dramatically in seven days.
Limb buds that were barely visible at 7 weeks now elongate. Upper limb buds show a paddle shape that will become the hand. Lower limb buds are slightly behind in development. The head is disproportionately large, occupying almost half the total length. The face begins to form: the lens placodes, which will become the eyes, appear as small dark spots. The maxillary and mandibular processes that will fuse into the upper and lower jaw are visible.
The midgut herniates into the base of the umbilical cord. This is physiologic gut herniation, a normal event at 8 to 10 weeks. The abdominal cavity grows too slowly to accommodate the rapidly elongating intestine, so the gut temporarily develops outside the body. It returns and rotates into its final position by week 12. Seeing herniation at 8 weeks is normal. Seeing it after 12 weeks may indicate an omphalocele.
The heart rate peaks at this stage, often reaching 170 to 180 beats per minute. Cardiac activity should be readily visible on transabdominal ultrasound by 8 weeks, though transvaginal imaging still provides superior detail.
What cannot be seen yet
Understanding the limitations of early ultrasound is as important as knowing what it shows. At 5 to 8 weeks, the following cannot be assessed:
- Fetal anatomy in detail. The four chambers of the heart, the corpus callosum, the diaphragm, and the fingers are not formed well enough to evaluate. Detailed anatomy scans wait until 18 to 22 weeks.
- Fetal sex. The external genitalia are identical in male and female embryos until about 11 weeks. Any claim of sex determination before 12 weeks is speculation based on the angle of the genital tubercle, a method with limited accuracy.
- Chromosomal abnormalities. The nuchal translucency measurement requires a crown-rump length of 45 to 84 millimeters, corresponding to 11 to 13 weeks and 6 days. Early ultrasound cannot replace first-trimester screening.
- Placental function. The placenta is visible as a thickened area of the gestational sac wall, but its efficiency and position relative to the cervix cannot be determined until later. A low-lying placenta at 8 weeks is meaningless because the lower uterine segment has not formed.
Summary: what to expect week by week
- Week 5. Gestational sac visible, 2–4 mm. Yolk sac appears by end of week. No embryo yet. Double decidual sac sign confirms intrauterine location.
- Week 6. Embryo appears, 2–4 mm. Cardiac activity begins, 90–110 bpm. If embryo ≥7 mm with no heartbeat, miscarriage is diagnosed.
- Week 7. Embryo 9–14 mm. Heart rate 120–160 bpm. Rhombencephalon visible. Amniotic cavity separates. Limb buds emerge.
- Week 8. Embryo 16–22 mm. Heart rate peaks at 170–180 bpm. Physiologic gut herniation appears. Lens placodes and jaw processes visible. Limb buds paddle-shaped.
Dating the pregnancy with ultrasound
Crown-rump length measured between 6 and 12 weeks is the most accurate method for dating pregnancy. The margin of error is ±3 to 5 days. After 12 weeks, dating by head circumference and femur length becomes less precise because individual variation in growth increases. If the ultrasound date differs from the last menstrual period date by more than 5 days before 9 weeks, the ultrasound date takes precedence. If the difference is more than 7 days between 9 and 14 weeks, the ultrasound date also prevails.
In pregnancies conceived via in vitro fertilization, gestational age is calculated from the embryo transfer date, not from the last menstrual period. A day-5 blastocyst transfer on January 1 corresponds to a gestational age of 2 weeks and 5 days on the day of transfer. The formula is transfer date plus 14 days for day-3 embryos, or transfer date plus 19 days for day-5 blastocysts.
When the scan raises questions
Early ultrasound sometimes produces findings that are inconclusive rather than diagnostic. A sac without a yolk sac at 5 weeks may simply be too early. A slow heart rate at 6 weeks may normalize a week later. A discrepancy between sac size and crown-rump length may resolve. The only way to distinguish a pregnancy that is too early from one that is failing is serial scanning 7 to 10 days later.
Guidelines emphasize caution. The International Society of Ultrasound in Obstetrics and Gynecology recommends that the diagnosis of early pregnancy failure be made only when strict criteria are met: mean sac diameter ≥25 mm without an embryo, or embryo ≥7 mm without cardiac activity. Anything short of these thresholds mandates follow-up.
Early pregnancy ultrasound is a tool of anatomy, not prophecy. What it shows at 5, 6, 7, and 8 weeks is the architecture of development — the structures that must appear in sequence for a pregnancy to continue. Each week answers a specific question, and each answer narrows the uncertainty. A full picture takes time.